Applications / Medical Devices
Surgical robotics: force feedback and backdrivability in piezo-driven tools
Solving the self-locking paradox for haptic transparency in miniaturized surgical instruments
Surgical robots extend the surgeon's hands into spaces too small, too deep, or too tremor-sensitive for direct manual access. The actuators in these robots must accomplish two seemingly contradictory tasks: drive the instrument with precision and force, and simultaneously transmit the feel of tissue interaction back to the surgeon's fingers. This second requirement, haptic or force feedback, demands that the actuator be backdrivable, meaning external forces at the instrument tip can rotate the motor shaft and be sensed at the input. Piezoelectric ultrasonic motors present both an opportunity and a challenge in this context. Their extraordinary torque density and compact size make them ideal for miniaturized surgical instruments, but their inherent self-locking friction, the same property that provides holding torque without power, resists backdrivability and complicates haptic feedback.
This article examines the force feedback requirements for surgical robots, explains the backdrivability challenge specific to piezoelectric motors, surveys the engineering solutions that have been developed, and evaluates piezo drives against conventional actuator technologies used in current surgical robot platforms.
Image: Physik Instrumente (PI)
Force feedback in surgical robotics: why it matters
The clinical case
A surgeon performing open surgery continuously senses forces through the instrument handle: the resistance of tissue being cut, the tension of a suture being tied, the compliance of an organ being retracted. This tactile information is processed unconsciously and guides the surgeon's force application in real time. Studies have shown that surgeons apply 40 to 60% less force variation (and therefore cause less tissue trauma) when haptic feedback is available compared to when it is absent.
The da Vinci surgical system (Intuitive Surgical), the most widely deployed surgical robot, famously lacks direct force feedback. Surgeons compensate using visual cues (tissue deformation, instrument deflection) and experience, but surveys consistently report that the absence of haptic feedback is the most-cited limitation of the platform. Newer robotic systems (Senhance by Asensus Surgical, Hugo by Medtronic, Versius by CMR Surgical) include some form of force feedback as a competitive differentiator.
Force magnitudes and frequencies
The forces encountered during surgical manipulation span a wide range:
| Surgical task | Typical force range | Frequency content |
|---|---|---|
| Tissue palpation | 0.1 to 5 N | DC to 5 Hz |
| Suturing (needle driving) | 1 to 10 N | DC to 10 Hz |
| Knot tying | 2 to 15 N | DC to 20 Hz |
| Tissue cutting (scissors) | 2 to 20 N | DC to 50 Hz |
| Grasping and retraction | 0.5 to 30 N | DC to 5 Hz |
| Tissue texture discrimination | 0.01 to 1 N | 5 to 300 Hz |
The force bandwidth requirement depends on the level of haptic fidelity desired:
- Gross force feedback (sufficient for preventing tissue damage): DC to 5 Hz, force resolution of 0.5 N. This captures the static and slowly varying forces of grasping, retracting, and probing.
- Fine force feedback (sufficient for suturing and knot tying): DC to 30 Hz, force resolution of 0.1 N. This captures the dynamic forces of needle insertion and thread manipulation.
- Texture discrimination (sufficient for tissue characterization): 5 to 300 Hz, force resolution of 0.01 N. This captures the high-frequency vibrations that distinguish healthy tissue from tumors, calcified vessels, or other pathology.
Most current surgical robots with force feedback target the gross or fine categories. Texture discrimination through a robotic linkage remains a research challenge, largely due to actuator limitations.
The backdrivability problem
What backdrivability means
An actuator is backdrivable if an external force applied to its output shaft produces a proportional and predictable motion or force at its input. In a backdrivable system, the surgeon feels the instrument-tip force transmitted through the robot's mechanical linkage and the actuator to the master controller. The key metric is the reflected impedance: how much force at the output is needed to produce a given motion at the input.
For a geared motor system, the reflected impedance is:
Z_reflected = J_motor x N^2 x s^2 + B_motor x N^2 x s + T_friction x N
Where J_motor is the motor inertia, N is the gear ratio, B_motor is the motor damping, T_friction is the friction torque, and s is the Laplace variable. The gear ratio N amplifies all three terms quadratically (for inertia) or linearly (for friction). A 100:1 gear ratio makes the motor feel 10,000 times more inertial and 100 times more frictional at the output.
A backdrivable actuator has low reflected impedance: low inertia, low friction, and low or no gear ratio.
The piezoelectric motor paradox
Ultrasonic piezoelectric motors generate output torque through friction between the vibrating stator and the rotor. This same friction, when the motor is not energized, creates a self-locking effect: external torques below the static friction threshold cannot rotate the shaft. The holding torque (the maximum external torque the unpowered motor can resist) is typically 2 to 5 times the continuous driving torque.
For a 30 mm diameter traveling-wave motor with 0.1 Nm continuous torque, the holding torque might be 0.3 Nm. To backdrive this motor, the external torque must exceed 0.3 Nm, meaning any tissue interaction force below this threshold is invisible to the system. At the instrument tip of a surgical robot with a typical mechanical advantage of 2:1 to 5:1, this translates to a minimum detectable force of 0.6 to 1.5 N, far too coarse for fine haptic feedback.
Even when the external torque exceeds the holding torque and the shaft begins to turn, the motion is nonlinear and unpredictable because friction transitions from static to dynamic regimes. The relationship between applied torque and resulting motion (or transmitted force) is not the smooth, linear function that haptic transparency requires.
This is the fundamental challenge: the property that makes piezo motors attractive for precision positioning (self-locking, no gearbox needed) is exactly the property that makes them problematic for force feedback.
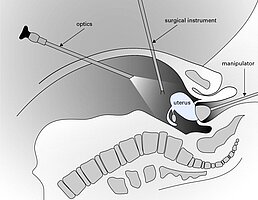
Image: Physik Instrumente (PI)
Solutions for haptic feedback with piezo motors
Solution 1: Active force sensing with force/torque sensors
The most straightforward approach bypasses backdrivability entirely. Instead of relying on the motor to transmit forces, dedicated force or torque sensors are placed at the instrument tip (or as close to it as practical), and the measured forces are displayed to the surgeon through the master controller's actuators.
Implementation: A six-axis force/torque sensor (such as an ATI Nano17, 15 mm diameter, 3.5 g) is mounted between the instrument wrist and the end effector. The sensor measures interaction forces with 0.01 N resolution and 1 kHz bandwidth. These measurements are transmitted to the master controller, which uses its own actuators (typically backdrivable BLDC motors) to generate the corresponding forces at the surgeon's fingertips.
Advantages:
- Completely decouples the haptic channel from the actuator's mechanical properties
- Works with any actuator type, including non-backdrivable piezo motors
- Can provide force scaling (amplifying or attenuating the displayed force)
- Can implement force limits (capping the displayed force to prevent surgeon fatigue)
Disadvantages:
- Adds mass and complexity at the instrument tip, where space is most constrained
- Force sensors are expensive ($1,000 to $5,000 for surgical-grade miniature sensors)
- Cable routing through the instrument shaft is challenging
- Sensor drift and calibration require attention
- Does not provide passive haptic feedback (the surgeon feels nothing if the electronics fail); the system must be designed so that loss of force feedback is detected and handled safely
Force resolution achievable: 0.01 to 0.05 N, exceeding the requirement for fine force feedback and approaching the threshold for texture discrimination.
Solution 2: Current/impedance-based force estimation
Piezoelectric motor drive current and impedance change with mechanical load. By monitoring these electrical parameters, the interaction force can be estimated without a dedicated force sensor. This is the piezo motor equivalent of current-based torque estimation in electromagnetic motors, but the physics is more complex.
Implementation: The motor driver continuously monitors the motional current (the component of drive current that produces mechanical work, separated from the capacitive current by circuit design or signal processing). The motional current is approximately proportional to the motor's output torque under steady-state conditions. Changes in motional current reflect changes in external load.
Advantages:
- No additional sensors or mechanism complexity
- Zero additional mass at the instrument
- Works with standard motor driver with added signal processing
Disadvantages:
- Force estimation accuracy is limited by the nonlinear friction characteristics of the motor
- Bandwidth is limited by the motor's mechanical time constant (typically 5 to 20 ms, giving 50 to 200 Hz bandwidth for the force estimate)
- Static forces (when the motor is not moving) cannot be estimated because motional current is zero at standstill
- Sensitivity is poor at low force levels (below about 10 to 20% of the motor's rated torque) due to friction variability
- Requires careful calibration that may drift with wear and temperature
Force resolution achievable: 0.2 to 1 N, adequate only for gross force feedback. Not suitable for suturing or tissue discrimination.
Solution 3: Controlled backdrivability through active drive modulation
This approach makes the motor partially backdrivable by actively modifying the friction interface. When the drive electronics reduce the stator vibration amplitude to near-zero, the contact pressure between stator and rotor decreases (in some motor designs, particularly those with axially preloaded stators), reducing friction and allowing some degree of backdrive.
Implementation: The drive electronics alternate between two modes:
- Drive mode: Full excitation, normal motor operation, high friction (self-locking)
- Sense mode: Reduced or zero excitation, lowered contact pressure, reduced friction, partially backdrivable
By cycling between these modes at a rate faster than the haptic bandwidth (above 1 kHz), the motor provides both driving capability and a degree of backdrivability in a time-multiplexed fashion.
Advantages:
- Uses the motor's intrinsic properties; no additional sensors
- Can potentially provide passive haptic feedback (the motor is partially backdrivable during sense phases)
Disadvantages:
- The achievable friction reduction is limited (typically 2 to 3x, reducing holding torque from 0.3 Nm to 0.1 to 0.15 Nm). The motor is still not truly backdrivable.
- Rapidly switching between drive and sense modes can cause audible noise and vibration at the switching frequency
- Control complexity is high; the system must maintain position control during the brief drive phases and measure deflection during the sense phases
- Not all motor designs permit significant friction reduction through drive signal modulation
Force resolution achievable: 0.1 to 0.5 N, marginally adequate for fine force feedback. Requires sophisticated signal processing.
Solution 4: Series elastic elements
A compliant element (spring) placed between the motor output and the instrument shaft allows the motor to remain in its self-locked state while the spring deforms under external forces. By measuring the spring deflection (with a high-resolution encoder or strain gauge), the interaction force is determined from the known spring stiffness.
Implementation: A torsional spring (typically a thin-walled titanium tube or a polymer flexure) with stiffness of 0.1 to 1 Nm/rad is inserted between the motor shaft and the instrument drive cable. A secondary encoder measures the angular deflection across the spring. Force is calculated as F = k x delta_theta x r, where k is the spring constant, delta_theta is the deflection, and r is the mechanical advantage.
Advantages:
- Provides true force measurement without expensive force/torque sensors
- The compliant element also acts as a low-pass filter, protecting the motor from impact loads
- Can be made very compact (a 5 mm long titanium tube adds minimal mass and length)
- Provides a degree of passive compliance, making the instrument inherently safer
Disadvantages:
- Reduces the system's position control bandwidth (the compliant element introduces a resonant mode)
- The position accuracy at the instrument tip is degraded by the spring deflection under load
- Must balance spring stiffness: too stiff and the deflection is too small to measure accurately; too compliant and position control is compromised
- Adds one sensor (the secondary encoder) and associated signal processing
Force resolution achievable: 0.02 to 0.1 N with a well-designed compliant element and high-resolution encoder. Suitable for fine force feedback and approaching texture discrimination capability.
Solution 5: Hybrid actuator architectures
Some surgical robot designs use piezo motors for the high-force, low-speed axes (instrument insertion and rotation) and backdrivable electromagnetic actuators (voice coils or direct-drive BLDC) for the low-force, high-bandwidth axes (wrist articulation). This partitions the design problem: the piezo motors provide compact, powerful drive where force feedback is less critical, while the backdrivable actuators provide haptic transparency where it matters most.
Advantages:
- Optimizes each axis independently
- Avoids compromising the piezo motor's strengths
Disadvantages:
- Increased system complexity (two actuator types, two driver architectures)
- The electromagnetic actuators must be MRI-compatible if the system is intended for intra-operative MRI (which negates the piezo motor's primary advantage in that context)
Comparison with conventional surgical robot actuators
Cable-driven BLDC (da Vinci architecture)
The da Vinci system uses BLDC motors located outside the patient, connected to the instrument tip through a cable/pulley transmission. This architecture provides:
- Backdrivability: Moderate. The cables have low friction but the pulleys and motor inertia create significant reflected impedance. The da Vinci system chose not to implement force feedback despite the partial backdrivability.
- Force capability: 5 to 15 N at the instrument tip
- Position accuracy: 0.1 to 0.5 mm at the tip
- Instrument diameter: 8 mm (standard) or 5 mm (reduced instruments), constrained by the number of cables that must pass through the shaft
- Sterilization: The instrument is detachable and steam-sterilizable; the motor unit is not sterilized
Direct-drive BLDC (newer platforms)
Some next-generation platforms place small BLDC motors closer to the instrument wrist, reducing cable lengths and improving bandwidth. These motors are typically 6 to 10 mm diameter and use either direct drive or low-ratio (5:1 to 20:1) gearing.
- Backdrivability: Good with direct drive; moderate with gearing
- Force capability: 2 to 8 N at the instrument tip (limited by motor size)
- Position accuracy: 0.05 to 0.2 mm
- Instrument diameter: 8 to 12 mm (the motors increase the instrument diameter)
- Sterilization: More challenging; motors near the instrument tip must survive sterilization or be single-use
Piezo direct drive
A piezo motor-driven instrument places the ultrasonic motor at or near the instrument wrist, driving the end effector directly or through a simple linkage.
- Backdrivability: Poor (self-locking); requires one of the solutions described above for force feedback
- Force capability: 5 to 30 N at the instrument tip (high torque density enables high force in small packages)
- Position accuracy: 0.01 to 0.1 mm (no backlash, high resolution)
- Instrument diameter: 5 to 8 mm (compact motor enables smaller instruments)
- Sterilization: See below
Quantitative comparison
| Parameter | Cable-driven BLDC | Direct-drive BLDC | Piezo direct drive |
|---|---|---|---|
| Instrument diameter (mm) | 5 to 8 | 8 to 12 | 5 to 8 |
| Tip force (N) | 5 to 15 | 2 to 8 | 5 to 30 |
| Position accuracy (mm) | 0.1 to 0.5 | 0.05 to 0.2 | 0.01 to 0.1 |
| Backdrivability | Moderate | Good | Poor (requires solutions) |
| Bandwidth (Hz) | 10 to 30 | 20 to 50 | 50 to 150 |
| MRI compatibility | No | No | Yes (with non-magnetic build) |
| Mass per DOF at wrist (g) | 5 to 15 (cables only) | 30 to 60 | 10 to 25 |
| Power per DOF (W) | 2 to 10 | 1 to 5 | 0.5 to 3 |
The piezo drive excels in force density, position accuracy, and miniaturization. Its weakness in backdrivability is the primary barrier to adoption in force-feedback surgical systems, but the engineering solutions described above can close this gap at the cost of additional complexity.
Miniaturization: the compelling advantage
The most powerful argument for piezo motors in surgical robotics is miniaturization. Smaller instruments enable less-invasive surgery: smaller incisions, less tissue trauma, faster recovery, and access to anatomical spaces that current instruments cannot reach.
Consider the design constraints for a 3 mm diameter instrument with two articulated degrees of freedom at the wrist:
- Available cross-section: pi x (1.5 mm)^2 = 7.1 mm^2. After subtracting the structural tube wall (0.3 mm thick), working lumen, and clearances, approximately 3 to 4 mm^2 is available for actuator mechanisms.
- Cable-driven approach: Requires at least 4 cables (2 per DOF) of 0.1 to 0.2 mm diameter, plus pulleys of 1 to 2 mm diameter. Feasible but with very limited force (under 2 N) and significant friction in the cable routing.
- BLDC motor approach: The smallest commercially available BLDC motors (4 mm diameter) would not fit inside a 3 mm shaft. Motors would need to be proximal, connected by cables, reverting to the cable-driven architecture.
- Piezo motor approach: Piezo linear motors (LEGS type or inchworm type) can be fabricated at dimensions of 1.5 x 1.5 x 6 mm, fitting within the 3 mm instrument shaft. These can produce forces of 1 to 5 N directly at the wrist joint, without cables or gearing.
This size regime (sub-5 mm instruments) is where piezo motors transition from being an alternative to being the only viable embedded actuator technology. For microsurgical applications (ophthalmology, neurosurgery, otology), this capability is transformative.
Specific examples
Ophthalmic microsurgery: Retinal membrane peeling requires forces of 1 to 10 mN applied with sub-10 um precision. Current instruments are passive (manually operated); tremor limits the surgeon's precision to approximately 100 um. A piezo-actuated instrument with integrated force sensing could provide tremor cancellation and force scaling, improving precision by 10x.
Cochlear implant insertion: Electrode arrays are threaded into the cochlea through a 1 to 2 mm opening. Insertion forces must be controlled to under 10 mN to avoid damaging the delicate intracochlear structures. A piezo-driven insertion tool with force feedback could maintain optimal insertion force throughout the procedure.
Endovascular intervention: Microcatheters navigating tortuous vessels benefit from steerable tips driven by embedded actuators. Piezo motors can provide the 0.5 to 2 N of tip force needed for steering within a 2 to 3 mm catheter diameter.
Sterilization compatibility
Surgical instruments must be sterilized between uses. The sterilization method depends on the instrument's material composition:
Steam sterilization (autoclaving)
The standard method: 134 C saturated steam at 2.1 bar for 3 to 18 minutes. This is the preferred method for reusable instruments because it is fast, reliable, and well-validated.
Piezoelectric motors can survive autoclaving if designed for it:
- PZT ceramic: Stable at 134 C. Thermal shock during the rapid heating and cooling cycle is the primary concern; PZT-8 has adequate thermal shock resistance if the ceramic thickness-to-diameter ratio is managed (thinner elements are more resilient).
- Adhesive bonds: Standard epoxies soften at 134 C. Autoclave-compatible adhesives (glass frit, silver-filled epoxy, or mechanical retention instead of adhesive) are required.
- Bearings: Ceramic bearings (Si3N4) with PEEK cages survive autoclaving without degradation.
- Electrical connections: Solder joints may fatigue under repeated thermal cycling. Welded or crimped connections are preferred.
- Moisture exposure: The steam atmosphere introduces moisture to the friction interface. Post-autoclave dry-out (heating to 60 to 80 C in dry air for 15 to 30 minutes) restores normal friction characteristics.
Published data shows that quality piezo motors designed for autoclave compatibility maintain greater than 90% of rated performance after 500 autoclave cycles, corresponding to approximately 2 years of daily-use surgical instruments.
Ethylene oxide (EtO) sterilization
Used for heat-sensitive devices. The motor is exposed to EtO gas at 37 to 63 C for 1 to 6 hours, followed by aeration. Piezo motors tolerate EtO sterilization without degradation, as the temperatures are well within the normal operating range and EtO does not attack the motor's materials.
Hydrogen peroxide plasma sterilization
Used for moisture-sensitive devices. Vaporized H2O2 at 45 to 55 C with plasma activation. Compatible with piezo motors; no material degradation observed.
Gamma irradiation
Used for single-use devices. Typical dose is 25 to 50 kGy. PZT ceramics are radiation-resistant to doses well above 100 kGy. PEEK and alumina are similarly resistant. Gamma sterilization is fully compatible with piezo motors and is the preferred method for single-use instruments with embedded piezo actuators.
Single-use versus reusable instruments
The economics of surgical robotic instruments favor limited-use models (10 to 20 uses before mandatory replacement). For piezo-driven instruments, this model aligns well with the motor's wear life: a motor rated for 3,000 hours of continuous operation at rated load will far exceed the 10 to 100 hours of total use accumulated in 10 to 20 procedures.
Single-use instruments with embedded piezo motors become economically viable when the motor cost drops below approximately $20 to $50 in volume production. Current costs for miniature piezo motors in medical-qualified form are $50 to $200, but declining with increased adoption and manufacturing scale.
The state of the art and the path forward
Current commercial systems
As of 2026, no major commercial surgical robot uses piezoelectric motors as primary joint actuators in the instrument. Piezo motors are used in several surgical systems for secondary functions (fine positioning, needle insertion, optical focus adjustment), and in MRI-compatible interventional robots where they are the only viable option.
Research systems
Academic and research labs have demonstrated piezo-actuated surgical instruments at scales from 3 mm to 10 mm diameter, with 2 to 6 degrees of freedom, and force feedback using several of the approaches described above. Key demonstrations include:
- Johns Hopkins APL: 5 mm diameter laparoscopic instrument with embedded piezo linear motors, 3 DOF wrist, 5 N tip force, series elastic force sensing with 0.05 N resolution
- EPFL: Piezo-driven microsurgical tool for retinal surgery, sub-10 um positioning, integrated force sensor, 10 mN force resolution
- University of Tokyo: 3 mm endoscopic instrument with piezo LEGS motors, 2 DOF, force estimation from motor impedance monitoring
Barriers to commercialization
Three factors currently limit broader adoption:
- Cost: Miniature piezo motors for surgical instruments cost 5 to 10x more than equivalent cable-driven mechanisms. This premium must be justified by clinical outcomes or capabilities that cable-driven systems cannot provide.
- Force feedback maturity: The solutions for haptic feedback with piezo motors (force sensors, series elastic elements, impedance estimation) add complexity and have not yet been clinically validated at scale.
- Regulatory pathway: Novel actuator technologies in surgical instruments face extensive regulatory scrutiny. The FDA and comparable agencies require demonstration of substantial equivalence or de novo classification, both of which involve significant time and cost.
Where piezo will win first
The most likely near-term adoption paths for piezo-actuated surgical instruments are:
- MRI-guided interventional systems: Here, piezo motors are already the standard because electromagnetic alternatives do not work. Force feedback is desirable but not strictly required for current clinical procedures (biopsy, ablation).
- Microsurgical instruments (sub-5 mm): Where miniaturization is the primary requirement and no alternative actuator technology fits the space envelope.
- Single-use instruments with embedded actuation: Where the instrument is simple enough (1 to 2 DOF) that the piezo motor cost is a manageable fraction of the disposable instrument price.
Conclusion
Piezoelectric motors offer surgical robotics a unique combination of high force density, compact size, zero backlash, and MRI compatibility that no other actuator technology can match. Their fundamental limitation, the non-backdrivable self-locking characteristic, is a genuine engineering challenge for force-feedback applications, but it is not an insurmountable one. Force/torque sensors at the instrument tip, series elastic elements, impedance-based estimation, and hybrid architectures each provide viable paths to haptic feedback with different trade-offs in complexity, accuracy, and cost.
The strongest case for piezo-driven surgical instruments is in the sub-5 mm size regime, where cable-driven mechanisms reach their practical limits and electromagnetic motors simply do not fit. As surgical practice moves toward smaller incisions, natural orifice access, and microsurgical precision, the demand for miniaturized, high-force, high-precision actuators will grow. Piezoelectric motors are positioned to meet that demand, once the force feedback problem is satisfactorily solved and manufacturing costs decline to the level that single-use instrument economics require.